Moderator Marlies Casier is the chair of the Be-cause health working group for Sexual and Reproductive Health Rights (SRHR) and as such the right person to manage this session during which an international panel looks at the impact of the climate emergency on SRHR.
Kim Van Daalen from Cambridge University did a scoping review on SRH in the context of climate migration. The finding results show that:
- Climate change reveals deeper questions of justice.
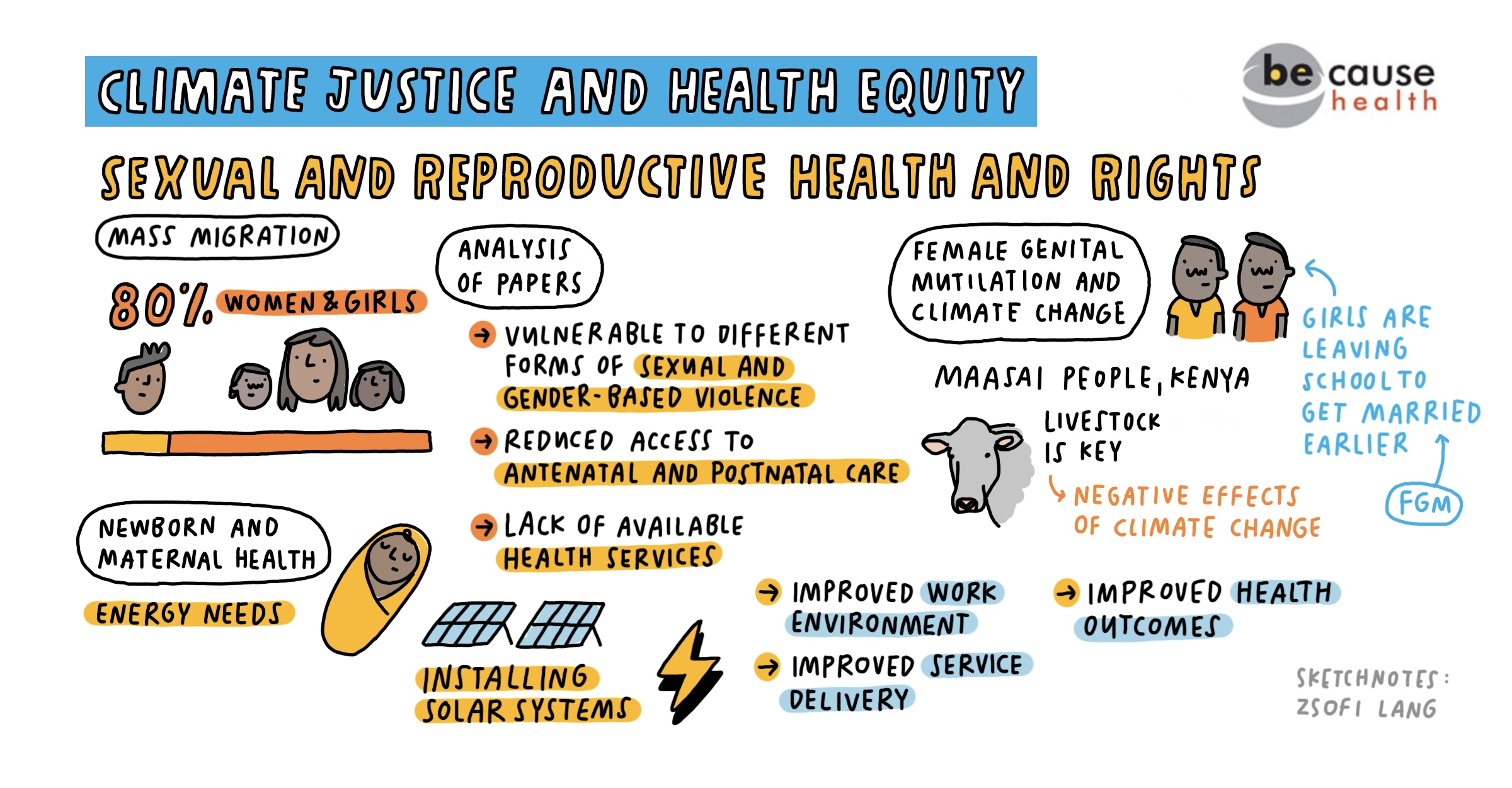
- Women and girls face increased climate induced health risks and experience unique SRH challenges during migration (for instance adverse pregnancy outcomes are increased by heat).
- In a climate migration setting, people are more vulnerable to Gender Based Violence (GBV).

"Climate change has increased gender inequalities among the Maasai [...] because lack of seasonal rain and subsequent droughts lead to crop failures [...] and increasing poverty."
Commonly cited recommendations to address SRH needs are:
- Gender responsive adaptation and mitigation policies.
- Increase the quantity and quality of empirical evidence on the effect of climate migration on SRH (climate-migration SRH nexus).
- A holistic and coordinated response.
Tammary Esho from AMREF Kenya conducted research on the intersection of Female Genital Cutting/Mutilation (FGM/C) and climate change among the Maasai in Kenya. Due to global warming, the areas where the Maasai live are affected by more frequent drought and unpredictable rains. The rising temperatures cause a fall in livestock, the main livelihood for the Maasai. The increasing poverty leads to more young women getting married earlier. Girls often have to undergo FGM/C before they can get married. Climate change is thus contributing to changes in the practices of FGM/C.
Gladys Ngeno, from Options, shares the results of a project in greening health facilities to improve maternal health and lower child mortality in Kenya. The unstable energy provision in health facilities in Kenya is a reality. An energy audit conducted in 60 health facilities at the start of the project reveals that although 75% of the health facilities were connected to the grid, only 3% had power back-up. This means that 97% of the facilities face an erratic supply of electricity (regular fall-outs lasting for about 6 hours) and hot water is often not available for the women.
Results of the project show that providing solar energy systems increase the quality of the work environment (health worker motivation), service delivery (immunisation coverage keeping the cold chain, increasing blood transfusion, ensuring availability of laboratory services, reduced referral of complications), and improved health outcomes (skilled birth attendance, reduction in obstetric case fatality ratio and perinatal mortality). At the same time, solar power reduces carbon emissions and saves money (high return of investment and low maintenance).
The session concludes that already existing challenges on SRHR are being aggravated by the climate emergency. The SRHR working group of Be-cause health will pay further attention to this interlinkage and follow up on the insights of this session.